Its been a very hard week. Started Saturday with terrible increased pain that called for more pain meds. On Wednesday night kath developed what we would later find out to be a nasty urinary tract infection. She was offered hospitalization a few times prior in the week and each time she said no. There was not much they could do in the hospital for pain management that we were not already doing at home. Why be in pain next to strangers in a small room. Better in her own space. It was not at all the case Wednesday night / Thursday morning. Maxing out every pain med we had as well as a strong sleeping sedative did nothing. I knew at 11pm when she could not pee she would have to go. She still did not want to. She was delirious from the fever and pain and was up for 48hrs straight. In her brief moments of lucidity at around 6am she realized it was time to go, and so we did. This time via ambulance. The community nurse insisted. It was the correct choice. There is no way I could have safely driven with her in the car in her feverish state– she was grabbing and reaching for everything in her dream state. Luckily all the dreams seemed pleasant to banal with only one or two moments where she was scared.
Seeing her taken away in the ambulance hit many emotional nerves. It was a new marker of where she is now for one…. And there is something jarring in the contrast of the calm and deliberate nature of the paramedics. They are there to do their job. They are kind and respectful but not emotional about what they do. My emotions on the other hand are high and it takes a lot of effort to not fall apart. I am a full bystander suddenly to this part of Kathleen’s journey. I stand aside as they put her on a chair and safety belt her in. It was raining and cool. They had waterproof blankets. They are of course prepared. Its routine for them. So I could feel slightly less separated, I held an umbrella over Kathleen as they took her to the truck. I could not go as I had to let Orville out who was crying as strangers took Kathleen away without her normal “Guard the house Orville, I’ll be back….” as she would throw a cookie to him. Will she come back ? Of course the thought is there. How can it not.
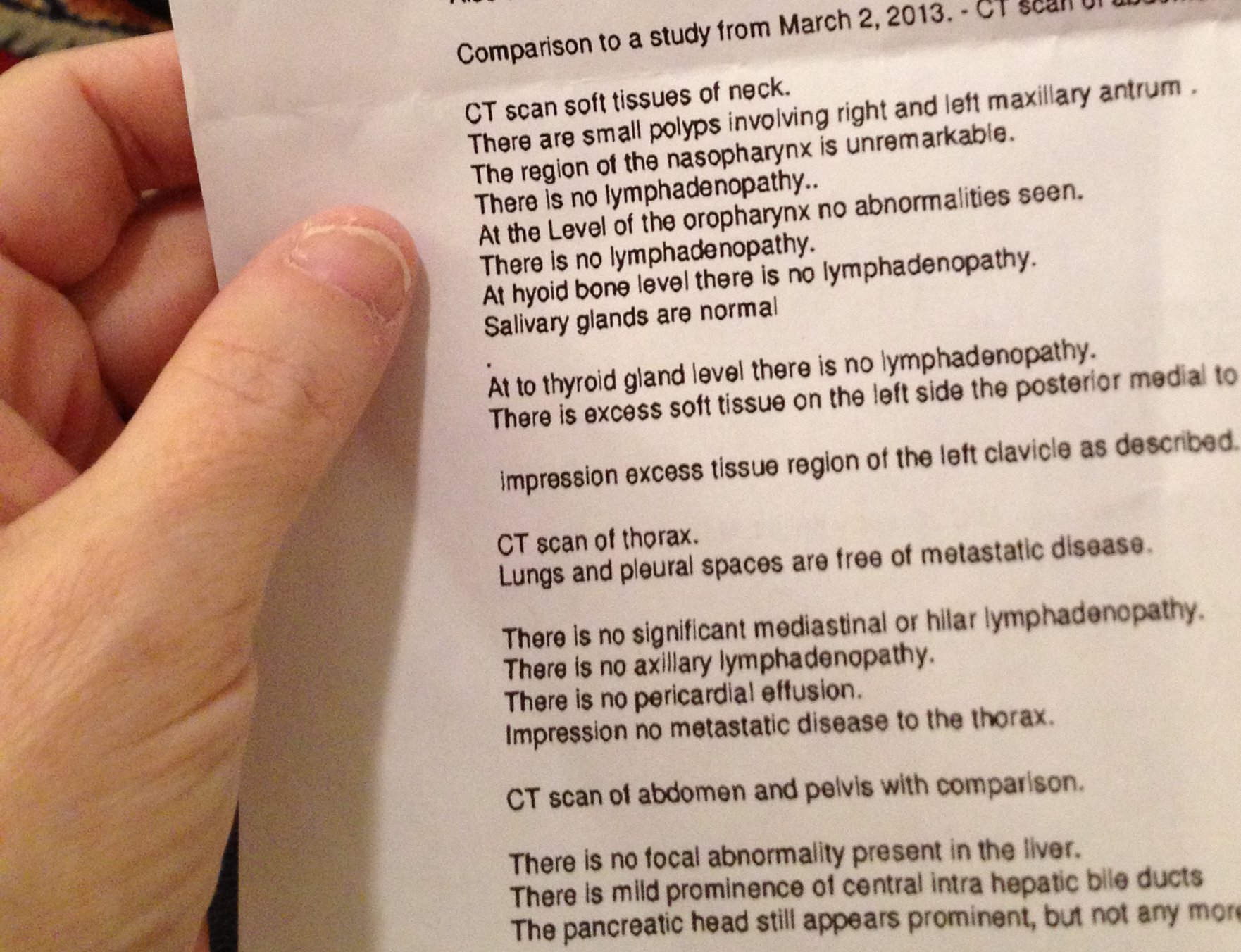
Emerge was fast. They are surprised that with all the meds, she still in so much pain. Even unconscious and unable to respond verbally, its clear she is in a world of hurt. As she was scheduled for a CT scan next week, they decided to do it right away instead to hopefully find the cause. Blood cultures show she has a nasty bladder/UT infection and her bladder is overly full. Cipro I.V. Since there was zero possibility she could lay still, they actually put her out and had an anesthesiologist with her. The images were good quality.
Two doctors, one from Pain and Symptom, and the other, the head of in patient oncology come to see her in emerge to treat her and get the ball rolling for admitting her. An hour or so later, the emerge doctor looks at the CT images and determines going up to in patient oncology is where she needs to be…. So up we go. She has insurance so she can get a double room instead of a quad. But if the inn is full so to speak, you go where there is space. A bonus! A single room! No room-mates!
By about 4pm, her body is finally starting to twitch and spasm less. But still not lucid. Her main chemo doctor comes by to discuss the CT. Normally a man of few words, his face says it all. Even he is shocked to see Kathleen in this state. Unfortunately, they showed at least one of the tumors in her abdominal cavity growing and “something new going on in her lungs”. Kath was suspicious this was happening in the last week or two. She was getting more nausea again and her psoriasis was coming back just like it was when the FOLFOX, the first line chemo drug, stopped working. From reading up on FOLFIRI and FOLFOX, this is a common trajectory for both. It works for a while and then it doesnt in ~75% of the cases for duodenal cancer patients. The Pain and Symptom doctors think that if she were to pull through this infection, then perhaps a month in her current state.
… and then the back pain. The awful back pain. Even with enough pain meds to fell an elephant, she was still writhing in delirious agony the whole night prior to admission. Probably the bladder infection didnt help either with the generalized swelling.
Heavily sedated now and the pain meds are not quite so maxed out and she is generally resting comfortably. She hasnt been conscious for more than a few seconds of recognition since Thursday afternoon. But thats the least worse choice for now. Awake in horrific agony. Or unconscious…. b) So, can anything be done for the pain ? A radiation specialist was in to talk to us. He is willing to do what we like. The problem is, what do we do. Without a target, its just a guess as to where to zap. She has some very tiny ‘abnormalities’ in her upper spine but its probably just regular old age disc wear. But generally nerve impingement there does not translate to where she feels the pain. To put Kathleen through the radiation, its at least 10-15min on the table with about 8 ‘transfers’ to get her there. This means a lot of pain. If they guess it right, and radiation doc thinks the odds are against it, it would be 10-14 days before she might have some benefit and a full 5-6 weeks before the pain from that one part of the spine would be gone…. But there would be potentially an initial pain flare before it got better and the doctors think she has perhaps 4 weeks? More pain for unrealized gain. No.
For a pain block procedure, we have the same limitations and then some. The big one being, Kathleen would have to be awake to let the doc know where the pain is and when it stops. Thats not possible.
Another thought the neurologist has is But thats treated with chemotherapy. There is no way Kath can tolerate that either and she is no longer responding to the systemic treatment.
We talked about what Kath would want done when things came to this stage. Its not like we worked out a large decision tree of every scenario in detail, but enough that I dont worry too much about making mortal decisions on her behalf. The staff here were great about encouraging us to talk about end of life decisions months ago and we did for the most part. We might have procrastinated a bit, but I think all is relatively clear. The doctors are pretty sure she will pull through the infection by Monday. The nurses I poll are mixed. Some dont think she will, some say too early to tell. In the mean time we wait.
Kathleen knows nothing yet of the latest scan. It will be hard to tell her… Will I be able to tell her ?
A friend sent me this link to a rather timely article
http://www.theatlantic.com/health/archive/2013/06/a-better-way-to-die/276724/
I like the poem in it.
10pm. Time to go home for the night. Someone is in the room with her constantly as she could do damage to herself. The people here are really, really, really amazing, so Elaine and I dont worry leaving at night. We can stay if need be, but we are not at that stage quite yet.
—Mike